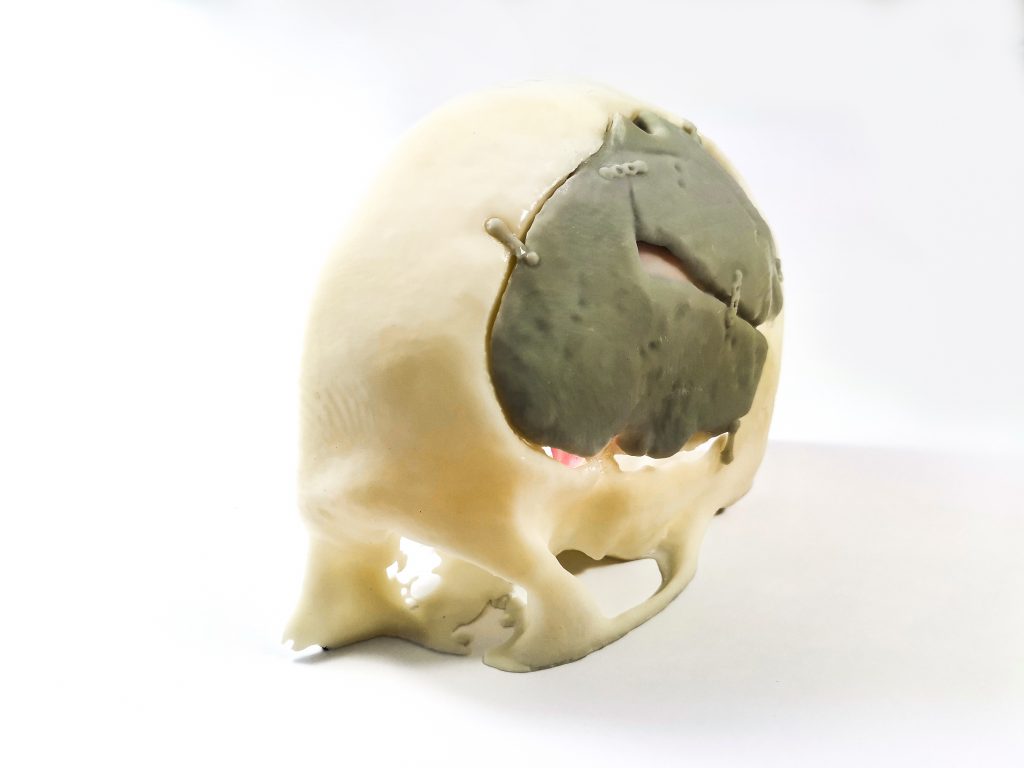
Anatomical biomodels used for surgical planning are 3D reconstructions, by software, of a patient´s anatomy from 2D images (CT, CBCT, MRI, etc.). Later, they are manufactured by 3D printing.
“After more than 30 cases, we have got used to having a 3D anatomical model in some surgeries, which are a little more demanding. The contribution of biomodels has become a basic need.” – Dr. David Santamarta Gómez.
The surgery is performed on a 71 years old patient with a convexity grade II meningioma, who had been intervened twice before. Both craniotomies differed in size and shape.
After the first one, the tumour had recurred within the resection margins. After the second intervention, the tumour had recurred again, approaching the midline.
In Dr. Santamarta´s words, the surgery was a completely success. The contribution of biomodels has changed the way surgical procedure is prepared. We are now closer to the task ahead. This particular case is one of the few which is not a skull base surgery.
Biomodels are considered, in many cases, as a valid alternative to the neuronavigator, as they bring you closer to the reality of the surgical process.
Consideration and fabrication of the biomodel
In every case, normally after a virtual revision with the surgeon, the roadmap is drawn up to obtain the final design. An initial, basic segmentation is performed to resolve the open questions the engineering team could have.
Production must fulfill the processes defined by Digital Anatomics, according to the regulations in the medical device field. So on, we can avoid posible mistakes and be more efficient, especially when we deal with highly complex models which combine multiple tissues.
Operation and results
In the words of Dr. Santamarta, the surgery was a success, the use of the biomodel contributed decisively to the planning of the intervention and to the design of the new craniotomy.
In many cases, biomodels are a valid alternative to the neuronavigator, as they bring the surgical process closer to reality.
Digital Antomics and biomodel manufacturing.
Our team consists of engineers with various backgrounds, including medical imaging, mechanical design and additive manufacturing.
The biomodel design process requires fluid comunication between surgeon and engineer, in order to become a true surgical planning tool.
This is not the first case of success by Dr. Santamarta. Previously, an olfactory groove meningioma surgery was planned with the assistance of our biomodels.
We are currently working on two new cases. The first one is a meningioma located in the greater wing of the left sphenoid, associated with hyperostosis of the sphenoid bone.
The second one is a plaque meningioma with injury at the appex of the right orbit, with hyperostosis of the right lesser wing of the sphenoid and the homolateral anterior clinoid apofisis.
Recibe las últimas noticias
¿Te gustaría estar al día en impresión 3D médica y novedades del sector?
Notificarme sobre los articulos
Receive the latest news
Do you want to be informed about the medical 3D printing sector and many other topics?